
Pregnancy is an important time of change, growth and stress, not only for the woman, but also for her partner, children and family (Duncan and Bardacke, 2010). The transition into parenthood can be perceived as a time of stress, which can be a catalyst for significant risks to health and wellbeing (Duncan and Bardacke, 2010). A systematic review examining the prevalence and course of anxiety disorders in men across the perinatal period concluded that a partner's pregnancy is one of the most anxious and stressful times that men experience (Leach et al, 2016). A lack of support for men during the perinatal period can exacerbate this anxiety and stress (Leach et al, 2016).
The emotional wellbeing of men with pregnant partners is central to supporting both the woman and the child (Bergstrom, 2013; Wynter et al, 2013). There is substantive evidence to show that high levels of stress are as prevalent for men as women in the perinatal period (Letourneau et al, 2012; BergstrÖm, 2013; Wynter et al, 2013). There is a paucity of literature, however, around specific antenatal programmes to support men in managing the stresses, life changes and challenges experienced both during their partners pregnancy and after the birth. One option for providing structured psychological support for men during the perinatal period, is training in the use of mindfulness techniques.
This integrative literature review examines the use of mindfulness-based stress reduction (MBSR) for men in the perinatal period, and discusses the applicability of MBSR for men with pregnant partners. The aim was to synthesise literature regarding the effectiveness of MBSR interventions used for men during the perinatal period and identify trends, themes and gaps in the literature. The review was guided by the question, ‘Can MBSR reduce stress in men with pregnant partners during the perinatal period?’
Mindfulness
MBSR has been shown to be effective in helping women to manage stress and anxiety during the perinatal period (Duncan and Bardacke, 2010; Goodman et al, 2014). Various adaptations of MBSR have been shown to be beneficial to both men and women in other areas of health, especially mental health (Bowlin and Baer, 2012; Bergen-Cico et al, 2013; Hall et al, 2016).
Mindfulness-based psychological interventions have been shown to be effective in reducing stress in various clinical and non-clinical populations (Grossman, 2008; Klainin-Yobas et al, 2012; Sharma and Rush, 2014); however, there has been scant research that investigates the outcomes of mindfulness-based interventions for men during the perinatal period.
Pregnancy presents a unique opportunity for midwives and health professionals to engage not only with the mothers-to-be but also fathers, using programmes that can have a positive impact on the family unit throughout the child-rearing years (Genesoni and Tallandini, 2009; Letourneau et al, 2011). Studies have shown significant links between the positive involvement and support of fathers and a reduction in maternal anxiety and depressive symptoms in the postnatal period and beyond (Sapkota et al, 2013). Men play a vital role in the support of their pregnant partners and the emotional development of their children; however, their emotional wellbeing and the support available to them is poorly understood within the context of becoming a father.
The aim of this integrative review was to synthesise literature regarding the effectiveness of mindfulness-based interventions for men during the perinatal period. There are no mental health screening or interventions (such as stress reduction or emotional management skills) targeted specifically to men with pregnant partners. This review reveals that MBSR programmes have the potential to benefit men in their transition to parenthood.
Data collection
Key search terms were derived from the guiding question and used in combination ‘Can MBSR reduce stress in men with pregnant partners during the perinatal period?’.
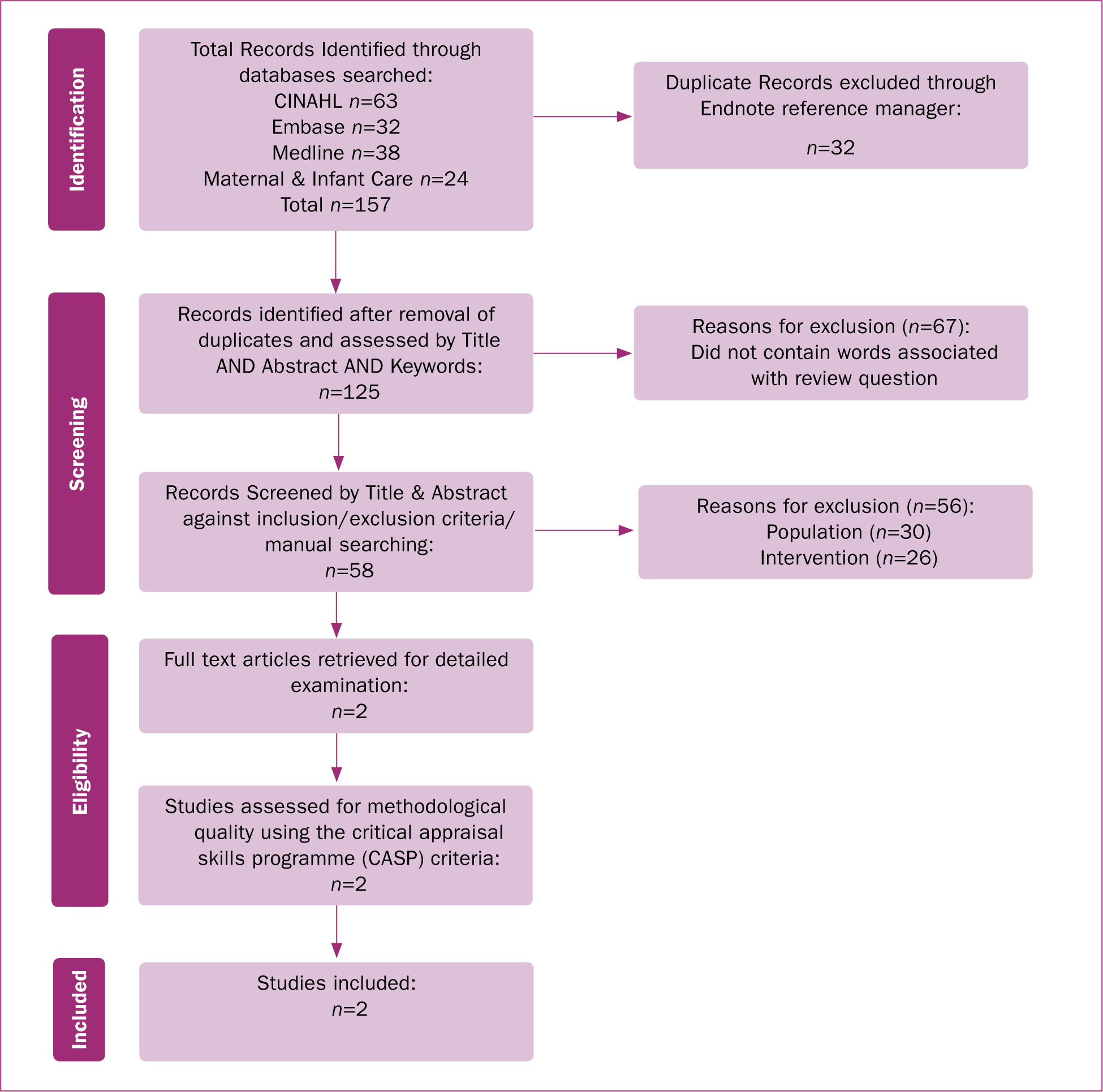
Searching of CINAHL, MIDIRS, Medline and Embase occurred with a combination of key terms: mindfulness, MBSR, insight meditation, stress reduction, mindful meditation, stress reduction, mindful meditation, emotional wellbeing, fathers, perinatal, pregnancy, dad, men and male, as well as manual searching of reference lists. The results of the search are detailed in Figure 1.
Results
Results from this review are presented as themes drawn from the two included studies and considered within the context of other relevant theoretical and research literature (Souza et al, 2010). Five themes were identified: variations in MBSR, essential ingredients of mindfulness, engagement of participants in mindfulness, measuring mindfulness, and mindfulness study limitations. The first three themes were discussed in Part I of this article (Jones et al, 2017). Part II will explore the latter themes identified.
Measuring mindfulness
In their mixed methods studies, Gambrel and Piercy (2015a; 2015b) used a number of measurement scales:
The outcomes of these measures, as reported by Gambrel and Piercy (2015a), indicated no significant differences between the treatment and control groups for the male participants pre-test quantitative scores. Men in the control group were found to have a significantly higher mindfulness total score than men in the treatment group at baseline (F(1,29)=4.84; P=0.04). No significant differences were found between the treatment and control groups on demographic characteristics, including age, race, length of relationship, marital status, educational attainment, length of partners pregnancy, and experience with mindfulness practice (Gambrel and Piercy, 2015a). Significant improvement was demonstrated for men in the MBSR treatment group for relationship satisfaction, F(1,29)=4.17; P≤0.05, and mindfulness F(1,29)=6.22; P<0.05 compared to those in the control group. No significant results were found for men for three measures of empathy (general, self in relationship, and partner in relationship), positive affect, and negative emotional states (Knabb, 2012). Quantitative measures for women demonstrated no significant variance for all outcome variables (Bergen-Cico et al, 2013). The following studies measuring mindfulness demonstrated similar findings in qualitative mindfulness measurements across a diverse range of populations and variables.
Quantitative measurements through validated tools
Gallagher et al (2010) examined the link between the level of aggression towards female partners, alcohol consumption and mindfulness. Male participants (n=167) were surveyed using the Mindfulness Attention Awareness Scale (MAAS) (Brown and Ryan, 2003). The results indicated that frequent alcohol consumption and lower levels of mindfulness were associated with an increase in aggression towards intimate partners. On the other hand, participants scoring higher on mindfulness were less likely to engage in aggression towards intimate partners. Gallagher et al (2010) suggested that mindfulness was a component in the reduction of aggression towards women by male alcoholics. This evidence suggested that mindfulness had a synergistic relationship with aggression that may be a modifiable risk factor in reducing aggression towards women (Gallagher et al, 2010). While this study is suggestive, limitations such as self-reporting on level of alcohol intake and the extent of intoxication at the time of aggressive episodes meant that the findings should be approached with caution (Gallagher et al, 2010).
Similarly, a study by Ghasemipour et al (2013), examining mindfulness and self-knowledge without intervention in relation to health-related variables, demonstrated that increased levels of mindfulness could contribute to improved health outcomes. Two groups of men undertaking mindfulness interventions were compared; group one with no known medical conditions (n=103) and the other group (n=101) with coronary heart disease. Ghasemipour et al (2013) found that the group with no known medical conditions had similar results as the group with coronary heart disease. Results obtained using the MAAS (Brown and Ryan, 2003) and the Integrative Self Knowledge scale (Ghorbani et al, 2008), Ghasemipour et al's (2013) findings are consistent with previous research by Grossman et al (2004), showing a correlation between lower mindfulness scores and an increase in mental health problems in men with coronary heart disease, according to the MAAS and Integrative Self Knowledge scale. The results indicate a link between lower levels of mindfulness and poor health outcomes (Ghasemipour et al, 2013). There is a growing body of evidence to suggest that lower levels of mindfulness are positively associated with poorer health outcomes and that mindfulness can improve health outcomes.

An experimental study by Hosseinzadeh Asl and Barahmand (2014) measured significant decreases in depressive symptoms in men who were drug dependent and treated with methadone. Participants (n=33, intervention group n=16, control group n=17) participated in a 2-hour weekly mindfulness intervention for 8 weeks. Pre- and post-test measurement was conducted using the Beck Depression Inventory II Scale (Beck et al, 1996). No significant difference was found between groups (P<0.05) in the pre-test, implying comparability of groups. The post-test scores, however, demonstrated significant differences in the control group (mean=23.65) versus intervention group (mean=16.94). Findings revealed that mindfulness interventions, used for depressive symptoms, lessened emotional distress and increased attention to thoughts and emotions, thus improving mental health (Hosseinzadeh Asl and Barahmand, 2014). However, the limitations of the study included failure to provide details of the methadone treatments and how this variable may have distorted the findings. Additionally, the health care providers involved in the methadone treatment programme recruited the participants; this may have created a power imbalance between the researchers and participants effecting outcomes measured.
Mindfulness interventions for men with prostate cancer have also been studied, showing reduced anxiety and fear associated with life threating illnesses. In a study by Chambers et al (2012), participants with prostate cancer participated in a 2-hour weekly mindfulness intervention for 8 weeks. Quantitative data were collected using the Hospital Anxiety and Depression Scale (Zigmond and Snaith, 1983), the Revised Impact Scale for Prostate Cancer (Roth et al, 2003), the Functional Assessment of Cancer Therapy Prostate (Cella et al, 1993) and the Five Facet Mindfulness Questionnaire (Baer et al, 2008). Measures were taken at baseline, after the intervention and at 3 months post-intervention (Chambers et al, 2012). The findings did not show any improvement in physical functioning or quality of life, which is consistent with the findings of a systematic review by Smith et al (2005), and a meta-analysis by Ledesma and Kumano (2009). The outcomes of the Chambers et al (2012) study indicated improvements in anxiety and fear as well as a marked usage of learnt mindfulness skills by participants, with the 3 month follow up reporting 54% of participants (n=7) undertaking regular formal mindfulness practices.
An randomised controlled trial by Gayner et al (2012) measuring mindfulness intervention (n=78) versus treatment-as-usual (n=39) for homosexual men with HIV, using a 3-hour weekly mindfulness intervention for 8 weeks, revealed positive results. Using standardised questionnaires, the Impact of Event Scale (Horowitz et al, 1979), the Hospital Anxiety and Depression Scale (Zigmond and Snaith, 1983), the Positive and Negative Affect Schedule (PANAS) (Watson et al, 1988) and the Toronto Mindfulness Scale (TMS) (Lau et al, 2006), the researchers established that improved mindfulness and reduced anxiety could be achieved through the use of the mindfulness intervention (Gayner et al, 2012). No statistical difference was present in the base line measures of the groups; however, PANAS and TMS scores showed marked improvements for the intervention group, which were sustained over a 6-month follow-up period. Interestingly, positive affect scores for PANAS were correlated with a decrease in anxiety and depressive symptoms (Kashdan and Breen, 2008).
Others have also noted how an increase in positive affect was correlated through quantitative measures with increased mindfulness (Davidson et al, 2003). Improvements in TMS scores reported in the Gayner et al (2012) study suggest that increased ability in mindfulness may be associated with improved coping with ongoing stressors and improved wellbeing. Limitations of the Gayner et al (2012) study include failure to describe ‘treatment-as-usual’ or to detail the use of antiviral or psychotropic medications for both the control and intervention groups. The results obtained by Gayner et al (2012) are similar to findings by Chambers et al (2012), in that measured mindfulness interventions had the potential to reduce anxiety and depressive symptoms, while increasing the ability to cope with stressors in men with terminal illnesses.
Biophysical quantitative measeurements
Quantitative findings obtained through validated survey tools demonstrate efficacy in the measurement of mindfulness, whether measured as an existing trait or as an intervention. Biophysical markers, such as stress hormones, have also been used to measure mindfulness. In studies by Bergen-Cico et al (2013), a reduction in cortisol levels occurred in men with post-traumatic stress disorder (PTSD) after participating in a 4-week mindfulness programme. Other biophysical changes have been measured using magnetic resonance imaging (MRI), including an increase in grey matter within the brain and the posterior parietal lobe, which is thought to be associated with mindfulness practices (Hölzel et al, 2011; Ives-Deliperi et al, 2013).
In a study of men with PTSD, Bergen-Cico et al (2013) examined the correlation between cortisol levels and mindfulness interventions. A randomised controlled trial was used to compare a mindfulness intervention (n=19) with treatment-as-usual (n=21). Participants in the intervention group received a 4-week mindfulness programme, with cortisol levels measured at baseline and completion. Analyses revealed a decrease in cortisol levels, associated with the number of mindfulness interventions undertaken. Participants in the intervention group displayed a reduction in waking cortisol levels (P<0.05), with cortisol levels below those of the treatment-as-usual group (Bergen-Cico et al, 2013). Measurement of salivary cortisol levels is directly indicative of blood cortisol levels and is considered a valid measure (Clow et al, 2004). Limitations of this study included small sample size (n=19) and the lack of post intervention follow up (Bergen et al, 2014). The inclusion of longitudinal baseline measurements of cortisol levels for veterans with PTSD would have also been beneficial in the validation of findings. Similar positive results were found in a longitudinal follow up study evaluating the use of MBSR in war veterans with PTSD (Kearney et al, 2012); however no cortisol levels were measured. Bergen-Cico et al (2013) suggested that mindfulness can be measured, and that a mindfulness intervention could contribute to reduced cortisol levels; a finding worthy of follow-up in a larger study. A similar study using cortisol biomarkers (Matousek et al, 2011), reported findings consistent with those of Bergen-Cico et al (2013), suggesting cortisol biomarker as an effective measure of mindfulness interventions.
Examining other quantitative measures of mindfulness interventions, Ives-Deliperi et al (2013) investigated the role of mindfulness in improving treatment for bipolar disorder. Outcomes were measured using functional MRI. Eight male participants underwent neuropsychological testing and functional MRIs before and after an 8-week mindfulness-based intervention. Half of the participants were wait listed, and tests were performed on both groups at the same intervals (Ives-Deliperi et al, 2013). The results were compared with a control group of healthy participants. Findings demonstrated changes in the prefrontal cortex region of the brain, with significant positive brain signal changes observed post-intervention (Ives-Deliperi et al, 2013). This suggests the possibility of measuring reductions in anxiety and improvements in emotion regulation for individuals with bipolar disorder through mindfulness interventions, which is similar to earlier findings of an randomised controlled trial (Williams et al, 2008). Investigations into changes in grey brain matter, as an outcome of mindfulness interventions or practices, are reporting significant positive results.
In their MRI study using a control (n=11) and intervention group (n=8) of male participants Hölzel et al (2011) were able to measure an increase in grey matter brain density among healthy individuals undertaking an 8-week mindfulness-based programme, pre-test compared to post-test. Additionally, the outcomes of the Five Facet Mindfulness Questionnaire (Baer et al, 2006) correlated positively with intervention group outcomes measured by MRI. No significant changes were noted in the control group (Hölzel et al, 2011). The authors concluded that increases in grey matter in the brain could be measured, demonstrating improved mental function and emotional regulation and indicating the effectiveness of MBSR as a behavioural intervention. Significant limitations of the Hölzel et al (2011) study included a failure to take account of exercise and group friendships occurring during the intervention period, which may also be related to significant increases in grey brain matter and wellbeing, thus confounding the outcomes of the study (Erickson et al, 2014).
Limitations of survey tools
Although empirical measures using MRI scanning and biomarkers such as cortisol afford a degree of validity when considering cause and effect in relation to mindfulness, the use of inventory survey tools for quantitative mindfulness measurements may have biases originating from the inventory developers. According to Grossman (2008), inventory tools have been developed by researchers with modest mindfulness experience or understanding of the practice's origins in Buddhist psychological theory. Grossman's (2008) underlying argument is that the usefulness of mindfulness stems primarily from direct personal experience with Buddhist meditation practices, and that researchers are unlikely to develop operational definitions that would reflect the concept of mindfulness beyond their own academic experiences. Grossman (2008) suggests that qualitative assessment based on interview data may afford a deeper and more accurate understanding of the multidimensional nature of mindfulness. Nevertheless, Gambrel and Piercy deem the concepts of using both quantitative and qualitative methods central to measuring mindfulness interventions in study populations (Gambrel and Piercy, 2015a).
‘Studying the effectiveness of mindfulness interventions requires the use of both quantitative and qualitative methods to fully understand the therapeutic use of this complex approach’
Qualitative measurements
Much of the literature on measuring mindfulness interventions for men mentioned in this review focuses on quantitative methods. Smith et al (2005) outline in their systematic review that there is a paucity of qualitative designs in the research of mindfulness intervention. While the vast majority of studies on mindfulness have been measured with quantitative tools, the participants perceptions, experience and satisfaction of mindfulness interventions is often under evaluated in mindfulness study designs (Smith et al, 2005).
In their second review paper, Gambrel and Piercy presented qualitative findings from 13 couples who had undertaken a 4-week MBSR intervention (Gambrel and Piercy, 2015b). This phenomenological investigation is the second part of a mixed methods study on MBSR for couples becoming first time parents. Quantitative results from the randomised controlled trial (Gambrel and Piercy, 2015a) demonstrated more significant results for men in relationship satisfaction, empathy and mindfulness scores compared to women. Seeking to understand the lived experience of the participants using phenomenological inquiry, Gambrel and Piercy asked the question ‘what are the experiences of couples in the mindful transition to parenthood programme?’ (Gambrel and Piercy, 2015b).
A total of 13 semi-structured interviews were conducted 1 week after the completion of the programme. These interviews lasted 45 minutes to 1 hour, with audio recordings being transcribed and printed (Gambrel and Piercy, 2015b). Data analysis included coding of the transcripts into categories to determine themes. The researchers then examined gender patterns from the codes and themes, allowing the experiences of both the men and women to emerge (McCown, 2013). Saturation was reached after ten interviews were conducted, but a further three interviews were included to expand the research record (Gambrel and Piercy, 2015b).
Four main themes emerged from the qualitative study (Gambrel and Piercy, 2015b): positive changes of self, improvements in couple relationship, being more prepared for baby, and male involvement. Positive changes of self was described as the ability to slow down and be more present, noticing increased acceptance and awareness of moments, and becoming less anxious and emotionally reactive (Gambrel and Piercy, 2015b). Men reported improvements in their relationships, such as greater connectedness with their partners, improved communication skills, and more insight into their partner's point of view. Participants believed these to be helpful tools in the maintenance of a positive relationship. Parents commented on feeling more prepared for baby, saying that the programme increased their confidence in their transition into parenthood. The negative effects associated with anxiety of this transition were minimised (Gambrel and Piercy, 2015b). The theme of male involvement describes the unique experiences of men when practicing mindfulness, which are not the same as those of their partners. Male participants believed that the programme allowed them to feel a deeper involvement with their partner's pregnancy, and that the programme helped them to connect with their baby while preparing to become a father (Gambrel and Piercy, 2015a; 2015b). Though there is a paucity of literature on MBSR literature for couples expecting their first child, and none for men in the perinatal period, the aforementioned studies demonstrate the ability of quantitative and qualitative studies to evaluate the outcomes of mindfulness interventions.
Mindfulness study limitations
Similarly to challenges faced by all researchers, Gambrel and Piercy were faced with balancing optimal design and feasibility (Gambrel and Piercy, 2015a; 2015b). In waitlist controlled studies, participants are generally randomised to receive the intervention immediately or after some time (Lindquist et al, 2007). During this delay, the control group receive care as usual, while the intervention group receive the treatment. Both groups are monitored and outcomes compared while the intervention was being implemented (Street and Luoma, 2002; Lindquist et al, 2007). The use of waitlists in randomised control trials has been criticised by Cunningham et al (2013) for artificially inflating intervention effect estimates. However, waitlists are common in studies investigating the effectiveness of new research interventions such as mindfulness (Gambrel and Piercy, 2015a; 2015b). Gambrel and Piercy also mention that although their sample was diverse in income, age, relationship status, ethnicity and religion, all the couples included in their study were skewed to being highly satisfied and considered highly educated. The authors suggested that this may have influenced the efficacy of the mindfulness intervention, leading to a ceiling effect (Gambrel and Piercy, 2015a; 2015b), and suggested the use of less satisfied couples in future studies. For the quantitative component of the study, a lager sample size would have increased statistical power. A significant qualitative limitation of the Gambrel and Piercy study was that participants were interviewed by the main researcher, who was also the group facilitator (Gambrel and Piercy, 2015b). As argued by Onwuegbuzie and Leech (2010), the relationship of participants to the interviewer may have unintended effects, such as participants being hesitant to be honest about negative aspects of the MSBR programme and/or declining to describe negative experience for fear of disappointing the interviewer. Conversely, it is also possible that, as the interviewer was known to the participants, they felt more comfortable sharing personal information due to the rapport that had already been established.
Discussion
This literature review demonstrates that studying the effectiveness of mindfulness interventions requires the use of both quantitative and qualitative methods to fully understand the therapeutic use of this complex approach.
This integrative review identified two articles from a single study of the use of MBSR for men in the perinatal period: one reporting quantitative findings and the other reported qualitative findings (Gambrel and Piercy, 2015a; 2015b). The two sets of findings were then examined, and five main themes emerged: variations in MBSR, essential ingredients of MSBR, engagement of participants in mindfulness and measuring mindfulness, and mindfulness study limitations. The first three themes were discussed in Part 1 of this article (Jones et al, 2017).
Quantitative methodologies employing validated measures have been used to collect data on the measurable effect of mindfulness interventions on a range of physical and mental health outcomes. Qualitative methodologies provide an opportunity to explore the human experience of mindfulness, including the acceptability of interventions for participants. A diverse range of male and female participants who experienced anxiety and stress related to various health problems reported similar beneficial outcomes from involvement in mindfulness interventions.
Given that the findings of studies using mindfulness interventions demonstrate the possibility to reduce stress and anxiety, applying a mindfulness intervention for men with pregnant partners appears feasible.
Conclusion
Exisiting literature on mindfulness interventions establishes positive outcomes across a range of clinical and non-clinical populations. Reductions in stress, anxiety and depression has been reported in both the quantitative and qualitative literature on mindfulness interventions.
Much of the quantitative research on mindfulness has been accompanied by limitations such as lack of randomisation and a control group, poor description of the target intervention, and small sample sizes. The findings of qualitative research on the use of mindfulness have suggested that, for participants, engagement with the intervention is brief, flexible and acceptable. Notwithstanding a number of methodological limitations, the studies reviewed indicated that mindfulness interventions for men did have a beneficial impact across a range of psychosocial health issues, including stress, anxiety and depression.
Studies of women during pregnancy indicate that mindfulness can be used to assist in the management of stressors that can become exacerbated in the perinatal period (Bergen-Cico et al, 2013; Fisher et al, 2012). However, there is a gap in the literature regarding whether mindfulness interventions can be used to support the emotion regulation and emotional wellbeing of men with pregnant partners. The findings of this integrative literature review suggest the importance of designing and evaluating a MBSR programme for the male partners of expectant women during the perinatal period.